Vascular Causes of Low Back Pain
Peripheral Vascular Disease
Peripheral vascular disease (PVD) affects both the arterial and venous systems and often times can lead to symptoms in the low back and lower extremities. The location of pain and symptoms is determined by the location of the pathology. Specifically when the aortic bifurcation is obstructed, a patient may report back pain alone or back pain with any of the following signs and symptoms (listed below). Symptoms are usually bilateral because the obstruction occurs before the bifurcation (division into the left and right common iliac arteries supplying each leg). However, when the iliac artery is obstructed, the patient is more likely to present with unilateral low back, buttock, and/or leg pain and numbness (of the involved side). Risk factors and signs/symptoms for peripheral vascular disease as a cause of low back pain are listed below.
Risk Factors
- Obesity
- Sedentary or inactive lifestyle
- Diabetes mellitus
- Hypertension
- Hyperlipidemia
- Older age
- Smoking
Signs and Symptoms
- Back pain (either alone or with any of the following symptoms)
- Unilateral or bilateral buttock and/or leg pain or discomfort (depending on where the obstruction is)
- Weakness and fatigue of the lower extremities
- Atrophy of the leg muscles
- Absent lower extremity pulses
- Color and/or temperature changes in the feet and lower legs
- Pain or other symptoms begin several minutes after the start of physical activity and resolve almost immediately with rest
Vascular or Neurogenic cause of LBP?
Low back pain due to vascular or neurogenic causes often occur within the same age group (commonly affecting individuals over the age of 60 years old). While vascular and neurogenic causes of low back pain can coexist within the same person, there are several major differences in these two distinct/different conditions that should be considered when differentially diagnosing the patient's cause of low back pain. Vascular causes of low back pain are often due to arterial occlusive disease which causes ischemia, discomfort, pain, and other symptoms depending on the location of the pathology (arterial obstruction). Neurogenic causes of low back pain are often due to spinal stenosis (a narrowing of the spinal canal, nerve root canals, or intervertebral foramina) which produces a resulting neurogenic claudication. The two columns below describe the main differences seen when comparing vascular- vs neurogenic-induced back and leg pain/symptoms.
Vascular-Induced Back and/or Leg Pain
- Symptoms are described as throbbing
- Patient may present with diminished or absent pulses
- Patient may present with trophic changes (such as changes in skin color, texture, or temperature)
- Activity (usually walking) brings on symptoms (within 1-5 minutes)
- Pain is present in all spinal positions
- NO symptoms with standing
- Pain/symptoms are alleviated by rest (usually within 1-3 minutes)
Neurogenic-Induced Back and/or Leg Pain
- Symptoms are described as burning
- Patient does not present with any change in pulses
- Patient does not present with trophic changes. Patient may however display subtle strength deficits (partial foot drop, hip flexor or quadriceps weakness, calf muscle atrophy)
- Symptoms are brought on immediately when the affected body part is used or when in certain positions
- Pain increases with spinal extension, decreases with spinal flexion)
- Symptoms PRESENT with standing
- Pain/symptoms are alleviated by changing the position of the spine and may respond to prolonged rest
One way that clinicians can differentiate vascular vs neurogenic causes of back pain is to conduct the van Gelderen Bicycle Test. The van Gelderen Bike Test helps assess for the underlying cause of intermittent claudication by looking at two important elements---the patient's response to rest and the position of the spine. Instructions on how to conduct the van Gelderen Bike Test are listed below followed by a supplemental video demonstration.
van Gelderen Bicycle Test Instructions
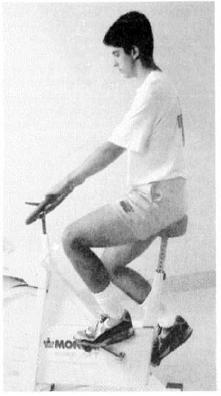
- Have the patient sit on an exercise bicycle.
- Instruct the patient to pedal against resistance without using the upper extremities (except for support). The patient should be in an upright position (lumbar lordosis and a slight backward lean if desired).
- After 5 minutes of peddling and observing, the patient's response is assessed. If there is pain or symptoms into the low back, buttock, or posterior thigh followed by tingling in the affected lower extremity then the first part of the test is positive. **NOTE: Whether the symptoms/pain are of vascular or neurogenic origin is still undetermined.
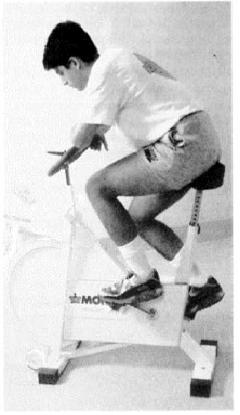
- The patient is then asked to lean forward and continue peddling (for 5 minutes). If the pain subsides over a short period of time, the second part of the test is positive for neurogenic claudication (but negative for vascular induced symptoms).
- The test is then confirmed for neurogenic cause of symptoms when the patient sits upright again and the pain/symptoms return.
Abdominal Aortic Aneurism
An aneurysm occurs when there is an abnormal dilation in a weak or diseased arterial wall causing a sac-like protrusion. Aneurysms can occur anywhere and in any blood vessels, but the two most common places are the aorta and cerebrovascular system. On occasion, an abdominal aortic aneurysm (AAA) can cause severe back pain. Prompt medical attention is imperative when detecting an AAA because an impending rupture is one of the most lethal clinical presentations, often leading to death. Information on the risk factors and signs/symptoms of an AAA followed by an instructional video on palpation and auscultation are listed below.
Risk Factors
- History of AAA
- History of vascular atherosclerotic disorders (vascular claudication, hypertension, vasculitis)
- Congenital Malformation
- History of cigarette smoking
- Positive family history
- Male Sex
Signs and Symptoms
- Palpable pulsating abdominal mass
- Mid-line lower thoracic/lumbar pain
- Pain descriptors: throbbing, pulsating, deep, boring
- Pain pattern: sharp, intense, severe, or knife-like in the abdomen, chest, or anywhere in the back
- Patient is unable to find a comfortable position
AAA Palpation Instructions
- Have the patient lay supine in a position of comfort, with the arms at the side, and the abdominal area exposed.
- Palpation should be done using the pads of the fingers and in a downward direction (using a gentle pressure towards the floor). Start palpating high in the epigastric area, feeling for the pulse.
- If a pulse is not palpated in this region, drop down lower following the linea alba, and again palpate for a pulse.
- Continue this process of feeling for a pulse until reaching the level of the umbilicus. If no pulse is palpated throughout this process, then palpation is negative for an AAA. If you feel a pulse at any level (from the epigastric region to the umbilicus) then the palpation test is positive for possible AAA. The clinician should then continue on to step #5.
- After a pulse is felt, outline the pulse between two hands. Keeping one hand on the outer edge of the pulse, palpate laterally to determine the presence of a laterally expansive pulsation. If this is present then an abnormal widening has occurred and the clinician should seek immediate medical attention.

{kind=link}
{kind=link}
{kind=link}